Brain Aneurysms Rupture While Receiving Physical Therapy
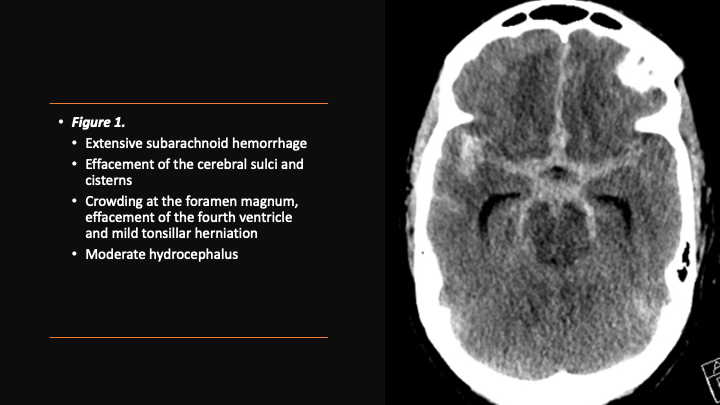
A 53 yo woman was in rehab therapy after a recent orthopedic surgery on her shoulder, when she suddenly lost consciousness while working with her Physical Therapist. She regained complete consciousness within a few minutes, however, she fell into a coma in the Ambulance on the way to the Hospital.
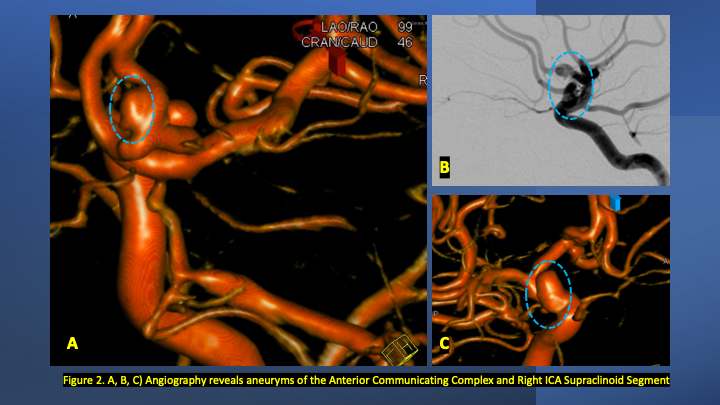
On admission, she presented as a GCS 3, was intubated, and stabilized hemodynamically in preparation for emergent catheter cerebral angiography, which revealed 2 discrete geographically located aneurysms – 1) Anterior Communicating and 2) Right ICA Supra-Clinoid Segment.
(Figure 2.)
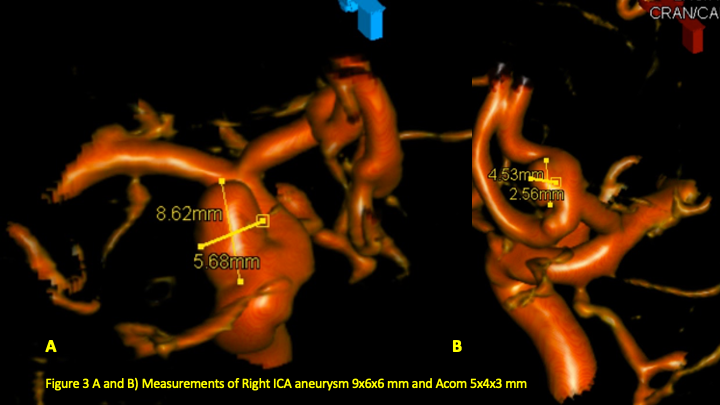
The Pattern of Hemorrhage was diffuse and generalized. On more careful analysis, however, there appeared to be focal hemorrhagic clot within the anterior inter-hemispheric fissure which raised greater suspicion for the Anterior Communicating Aneurysm as the source of hemorrhage. Although Acom Aneurysm was smaller, it’s irregular shape and eccentric “nipple” suggested potential rupture point. (Figure 3.)
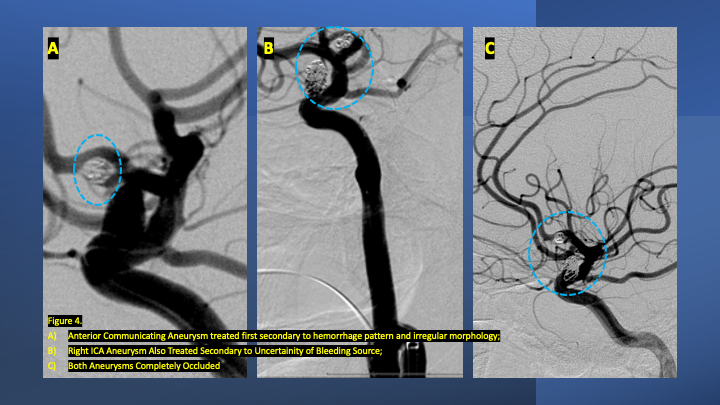
After careful measurements of the parent vessels, aneurysm sac, and aneurysm neck, we decided to proceed with Primary Coil Embolization of the Acom Aneurysm first, followed by the Right ICA Aneurysm next. Despite greater suspicion in the Acom region, a significant level of Uncertainty remained, and we felt it was better to secure both Aneurysms if capable of being performed safely. (Figure 4.)
After both aneurysms was secured, she spent 14 days in the Neurointensive Care Unit where she was monitored and treated for hydrocephalous and vasospasm. As a high-grade subarachnoid hemorrhage (WFNS Grade 4) patient, she underwent extensive critical care to manage cardiac, respiratory, DVT, seizure, and ID prophylaxis and treatment. During that period, she regained levels of consciousness, alertness, and neurologic function. Upon hospital discharge, she had regained all neurological functions, however remained globally weak and deconditioned. After 1 week in Acute Rehabilitation, receiving extensive physical and occupational therapy, she was able to return Home, where she was independent and returning to all her Activities of Daily Living at 1 month following her rupture event, mRS of 0.
Discussion:
The sudden onset of Coma can be from many causes, of which brain hemorrhage or stroke remain at the top of any list. That our patient was undergoing Physical Therapy for a shoulder surgery was unlikely to be directly related to our patient’s aneurysm rupture. Although intense physical exertion has been suggested as a risk, as have several other “Trigger” factors including coffee, cola, anger, startling, straining, nose-blowing, and sex.[i] This study was a well-executed Case Cross-Over Study of 250 patients in the Netherlands, however, is limited by Recall and Selection Bias. Specific recommendations for known unruptured aneurysm patients remain inconclusive and controversial.
The natural history of untreated ruptured brain aneurysms is very poor, with the classically quoted Finnish Study from the 1960’s of untreated ruptured intracranial aneurysms (RIAs) of 116 hospitalized patients reporting a 1-year mortality of 63%.[ii] A more recent Study from Helsinki University Hospital reviewed their Aneurysm Registry of 6850 patients between 1968 and 2007, of which 510 patients were classified as untreated and stratified into generational epochs. “During a lifelong follow-up of 510 untreated SAH patients, the 1-year mortality rate was 65%, 5-year mortality 69%, and 10-year mortality 76%. Hospital-admitted poor-grade patients with untreated RIAs had 1-year mortality rates of ≈90%. The 1-year mortality rate was 75% for good-grade patients admitted within a week. In theory, today’s patients, who are admitted within a week after SAH and who are not in poor condition on admission, have an ≈25% possibility to survive a year if treated conservatively.”[iii]
Early treatment of RIAs is highly recommended to prevent acute catastrophic rebleeding events. Landmark studies, specifically the prospectively randomized trial of 2143 patients, the International Subarachnoid Aneurysm Trial (ISAT), has demonstrated the short and long-term success of Endovascular Coiling in improving mortality rates and reducing the risks of rebleeding from the treated aneurysm. At 5 years, 11% (112 of 1046) of the patients in the endovascular group and 14% (144 of 1041) of the patients in the neurosurgical group had died (log-rank p=0.03), but the proportion of survivors at 5 years who were independent did not differ between the two groups: endovascular 83% (626 of 755) and neurosurgical 82% (584 of 713).[iv]
Endovascular coiling has gained acceptance as a primary approach to most ruptured brain aneurysms, however, a multi-disciplinary approach including surgical clipping, vasospasm prevention/therapy, hydrocephalous management, and advanced neurocritical care remain essential tools in the armamentarium of experienced neurovascular teams caring for these critically ill patients.
References:
[i] Vlak MH, Rinkel GJ, Greebe P, van der Bom JG, Algra A. Trigger factors and their attributable risk for rupture of intracranial aneurysms: a case-crossover study. Stroke. 2011 Jul;42(7):1878-82. doi: 10.1161/STROKEAHA.110.606558. Epub 2011 May 5. PMID: 21546472.
[ii] Pakarinen S. Incidence, aetiology, and prognosis of primary subarachnoid haemorrhage. A study based on 589 cases diagnosed in a defined urban population during a defined period. Acta Neurol Scand. 1967; 43(suppl 29):21–128.
[iii] Korja M, Kivisaari R, Rezai Jahromi B, Lehto H. Natural History of Ruptured but Untreated Intracranial Aneurysms. Stroke. 2017 Apr;48(4):1081-1084. doi: 10.1161/STROKEAHA.116.015933. Epub 2017 Mar 1. PMID: 28250196.
[iv] Molyneux AJ, Kerr RS, Birks J, Ramzi N, Yarnold J, Sneade M, Rischmiller J; ISAT Collaborators. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. Lancet Neurol. 2009 May;8(5):427-33. doi: 10.1016/S1474-4422(09)70080-8. Epub 2009 Mar 28. PMID: 19329361; PMCID: PMC2669592.